Comment Below

minute read
The Post Millennial wrote about the World Professional Association for Transgender Health conference in Montreal, Quebec, in September. We wrote about the panels at that conference, and what clinicians and activists were saying on those panels, including one on "Navigating The Changing Landscape With Littles And Their Families: Exploring The Role Of Mental Health Across Different Practice Settings With Transgender And Gender Diverse Pre-Adolescent Children."
As a result, The Post Millennial received a legal demand from Children's Minnesota, which publically available information states is the seventh largest pediatric health system in the United States, and advertises as “The Kid Experts.”
WPATH is an international non-profit organization which describes itself as being devoted to transgender health, and The Post Millennial intended to inform readers as to what is going on in the world of trans-affirming mental health care for prepubescent children. It turns out that, according to the panelists, it's an exciting, and burgeoning field. Clinicians from California, Minnesota, and Washington sat on the panel to discuss how they therapeutically treat prepubescent children, including those who are only just verbal, on gender transition.
In response to our news story, which contained a video of the panel as well as a record of the panelists names and their clinics, which they noted at the beginning of the panel, Children's Minnesota, the clinic where the moderator works, reached out to The Post Millennial via an in-house attorney.
Children's Minnesota demanded that the article be deleted from The Post Millennial's website. They did not want the video of the panel where clinicians discussed the medical and therapeutic gender transition of young children to receive broader public attention. We have not deleted the article. The Post Millennial believes that the footage meets every criteria of fair use.
The letter they sent to The Post Millennial stating that the article about the panel "disclosed identifying information of WPATH panelists... without proper consents." The information they objected to was provided in person at the conference, as well as via a live stream of the panel. Children's Minnesota claims that this was a violation of the WPATH Code of Conduct policy. This policy states that "Where applicable, photography, recording, or reproduction of any kind is not permitted without the explicit consent of any person and/or of the author/presenter/copyright- holder(s) of the material being photographed, recorded or reproduced." As such, they claim that our reporting is in violation of the Code of Conduct. After this letter, The Post Millennial took down the video of the full panel and replaced it with a three-minute clip.
The letter was sent by Michael Waldrop, Associate General Counsel for Children's Minnesota, which claims as its mission to "champion the health needs of children and families. We are committed to improving children’s health by providing the highest-quality, family-centered care, advanced through research and education."
Children's Minnesota has a gender clinic, as do many other hospitals across the US, such as Golisano Children's Hospital in Rochester, NY, Columbia University Medical Center, Boston Children's Hospital, Vanderbilt in Nashville, Seattle Childrens, and many more. Children's Minnesota offers confidential gender conversations for children over 10, puberty blockers for children who have already begun the Tanner stage 2 phase of development, and access to cross-sex hormones at about 15 or 16. To begin the process of taking hormones, "a letter of support is required." Fertility preservation is offered as well, since puberty blockers and cross-sex hormones lead to sterility.
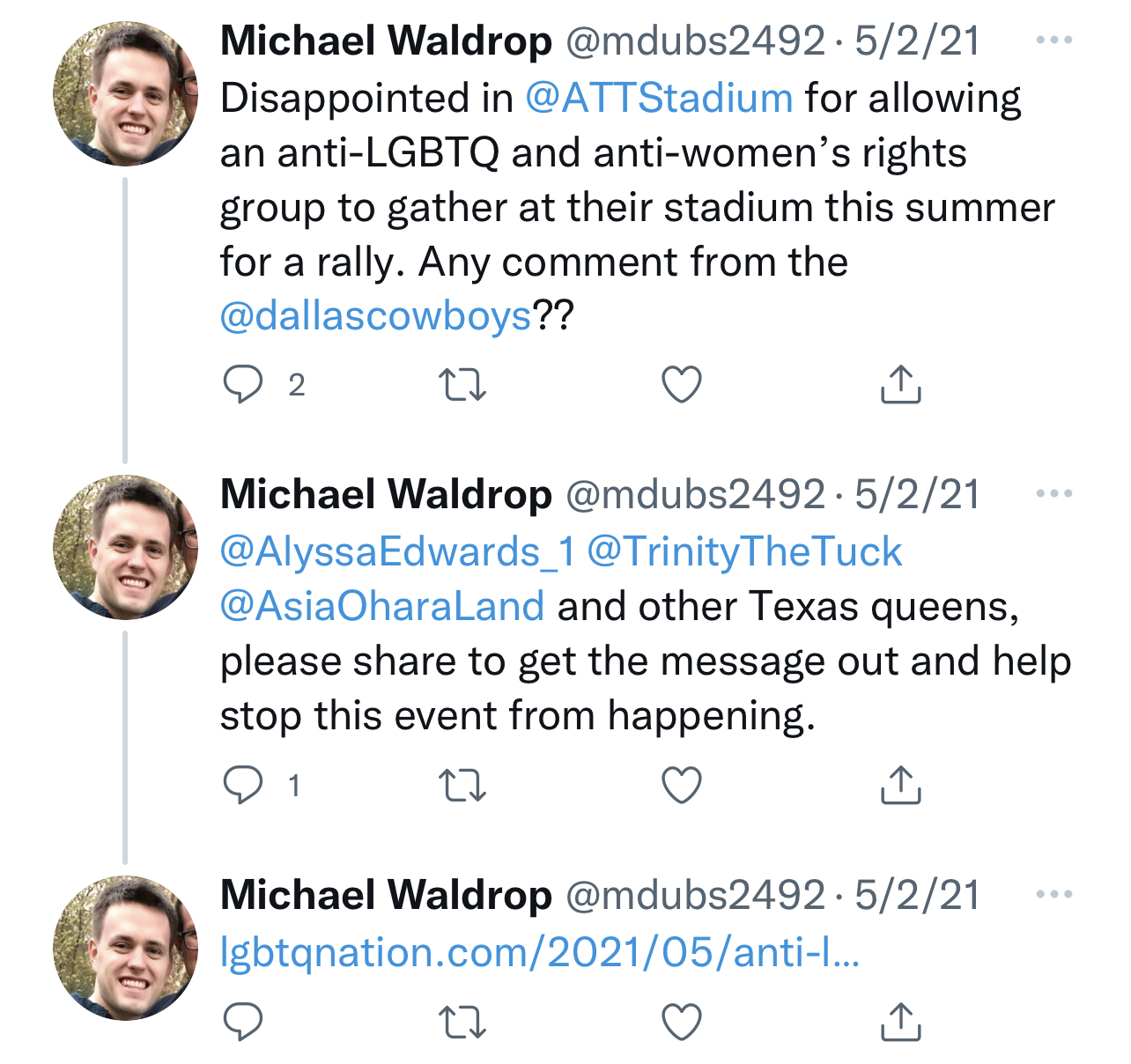
The in-house lawyer making the demand against The Post Millennial on behalf of Children's Minnesota, has been active in social media, including taking to Twitter in 2021 to chastise AT&T Stadium in Dallas for allowing the Christian men's group the Promise Keepers to host an event at the stadium. He asked for "Texas queens" to help "stop this event from happening."
Waldrop sent the letter on behalf of Children's Minnesota, presumably because the moderator of the WPATH panel worked at the institution. He was one of four panelists discussing the medical and therapeutic gender transition of children, and gave each panelist an opportunity to introduce themselves at the beginning of the panel, which they did. Waldrop did not immediatley respond to a request for comment from The Post Millennial.
The speakers on WPATH's panel on "Navigating The Changing Landscape With Littles And Their Families: Exploring The Role Of Mental Health Across Different Practice Settings With Transgender And Gender Diverse Pre-Adolescent Children" are clinicians who are excited to work in the burgeoning field of child gender transition. They note that what they call "gender care" began with adults, then branched out to teenagers, and is only now just beginning with children. For these providers, this is a new and exciting space in which to be working.
The panelists are mental health providers, working with children they call "gender expansive," they engage in play with those children during sessions to better understand that gender expression. Yet they don't feel that little kids need therapy for what may be termed "early onset gender dysphoria." Instead, one clinician said that mental health support is provided only as needed, and that usually it is needed not due to gender dysphoria, but because of the social stigma of trans. In other words, it's not the family seeking mental health treatment for a child who plays with supposed opposite-sex toys that's the problem, it's the rest of us.
"The pathology isn't being trans," says one provider, "the pathology is the transphobia that the kids and their families are winding through the world with. And so we're there as a mental health support if that causes really normal stress."
The focus for this clinician is on "helping families—and kids—feel like they can navigate the world with as much confidence, happiness, joy and groundedness as possible."
This, too, is the take of the Columbia University gender clinic, which takes the approach that the mental health issues surrounding the feeling of being born in the wrong body are the fault of society not being accepting enough of people who believe they are born in the wrong body, and not a mental issue with the person experiencing the dysphoria.
A provider who identifies as non-binary, transmasculine and bisexual, agreed with this assessment, saying that much of the work done at their clinic is "parent support and education stuff, too."
This is true "especially when you have two parents that cannot agree on what should happen, that can be like a really tricky situation."
These kinds of "tricky situations" are happening across the country, as one parent dons unicorn glitter pins and rainbow t-shirts, while the other makes the claim that a little girl playing with a toy truck doesn't make her a boy. It is often the more progressive parent that doesn't take the child's interests at face value, and determines that those interests are an indicator of actually, interally being the opposite sex.
Activists have successfully made the switch over the past few years between biological sex and gender identity, and have claimed that gender identity is innate, while biological sex is a social construct. Of course, feminism, where much of this begins, would posit that exactly the opposite is true.
The clinicians reference Dr. Rachel Levine, keynote speaker at the conference, who said that much of the work of trans advocacy and trans medical care was "suicide prevention." The idea has been put forth, with authority, that if children and teens are not permitted to undergo social and medical transition, they will simply kill themselves.
One clinician said that the reason she wanted to work with children was to cure the problems she saw in trans adults. "I worked with so many adults who described their childhood in ways that were very pathologizing, and stigmatizing," she said.
"And out of that they developed a lot of the things that we see happening," she said, "and I really wanted that to be prevented, and not even just prevented, but actually, like, celebrated and, you know, try to really have children, and adolescents be proud of who they are."
The nonbinary, transmasculine clinician uses themselves as an example to kids, and uses their "lived experience" in providing therapy to kids and families.
"I feel lucky to be like in kind of a unique position as a trans clinician to like, be there for the trans kids not just to show like you can grow up and like, have a life and stuff. But then their parents to also get to see like, 'oh, this person is like, professional, sort of.' And then they maybe be less likely to just like dismiss what I have to say, because of the lived experience. Which could also go the other way, sometimes I think."
When doing intake with a "trans kid," this clinician will "want to know about what their goals are that they've identified so far for transition, who's supportive of it? How is it going at school? What our extended family doing?"
Another clinician in Minnesota said that parents are the ones who are signing up their kids for these services. "Kids don't sign up for therapy themselves usually," she said, "so I have usually, really invested parents and kids that have persistently, consistently across many settings been presenting as gender diverse, gender, non binary or trans." She digs into the familiy relationships, and "does alot of drawings, and "sitting on the floor and playing and of course, even with littles I do have time with just the kid so that they can express themselves separate from their families."
She lets parents express their concerns as to their "own transition," and express their "grief" as well. The assumption is that once a child lands in gender care, they are trans, they must be affirmed, parents must adapt to this new reality, even if it has only been perceived by parents watching their kids play with opposite sex toys, or not wanting to wear clothes typically worn by children of their sex, or perhaps just because they like rainbows.
A clinician will often have child patients referred to them by a pediatrician, saying that "a pediatrician is screening for gender diversity within their clinic. And then if the child is expressing some gender diversity, they would refer them to our clinic."
She notes that "something the parents will, the parents always have given approval for that, but they don't always know what the means or who we are or what we're going to do together." Social workers are then sent in to call families and "explain the clinic."
They ask parents their goals for care prior to seeing them at all. And these clinicians make determinations about the family prior to that first appointment. Prior to intake, they "get a sense for where the child and family are at with a kind of understanding their child's gender and what goals they might have for that initial appointment with us."
"That kind of helps prepare us to know what type of room we might be walking into when we see a family for the first time. And then we can differentiate that intake depending on where the child and family are at," she said, noting that this determines whether they treat the child's family as hostile or supportive of gender transition.
"So it might be that we have a really supportive family. And in that case, we're spending time with the child and the family together talking about goals, or we might be that the child and the family are in really different places," she said, in which case they separate the child from the family and encourage the child to be proud to be trans, while reeducating the parents on why gender transition is suicide prevention, or why they need to express and get over their grief, or tell them ways to support their trans child.
"We need to spend a lot of time with the parents for that initial appointment, learning about their fears and concerns and providing a lot of psychoeducation to them at that time," she said.
One clinician does not that "non medical options for some children can be just as affirming as a medical one," and states that not all kids need to go on drugs to be who they truly are.
Another talks about playing games on the floor with kids and discussing fertility issues with them, or telling them not to be afraid of shots.
A clinician from Minnesota spoke about how the role clinicians play with parents, and "being able to correct misinformation." This nonbinary transmasculine therapist related an anecdote in which they told a parent about puberty blockers for their child, and said that therapists should not feel "reluctant to talk about medical stuff" despite not being doctors.
"The other day," they said, "I was talking to a mom and I was like, 'you could try, you know, blockers, you kind of hit the pause button while your kid thinks about it.' And she was like 'you can do what? Oh my God, perfect!'"
The clinician related that they thought "this is a bummer that this had not been like give to you before."
They also spoke about their role in schools, with children's extended family, and their community, and how caregivers can advocate for their "trans kids" across all these areas.
The therapist on the panel determined that she wishes it were possible to "diagnoses the whole family system," especially, she said, when working with kids who are only "recently verbal or just young."
"I do give space for families to work on their own grief and loss around what they thought when they named their kid the name that will not be their name anymore," she said. "And I work with families a lot on their fears for the child because again, what's pathologizing is the transphobia that they're navigating in the world with.
"And so they have some real huge fears. Like they read some article about suicidality and they're like 'my kid's now going to commit suicide.' And so a lot of it is about How to make sure that they're getting support accurate information and really connecting with other families," she said.
She recommends "doctor shopping" for parents when kids are pre-pubertal so that they can begin the medical gender transition process.
She also helps parents figure out how to "go to the school and ask for the right bathrooms," how to "tell the teacher to get the pronouns right," and how to get the child on a sports team based on their gender identity and not their biological sex. She tells parents how to advocate for legal name change, birth certificate change, both in ways that the child does not experience any undue stress. As for grandparents who just don't understand, she said that it's important to figure out "which grandparents love them and which grandparents don't."
She addresses some the medical problems of puberty blockers, saying that fractures could be a problem as bone density decreases as a result of halting the body's natural process, but suggests the kids should just play sports anyway.
One of the Minnesota clinicians emphasized "the importance of like teaching parents how to advocate at school, saying that this is "very important. And it feels like if we are not having them do it, then it's just by not doing it, then the kid is like having to do it. And being really clear with them, like if they're not taking on this emotional labor and work then they're just kind of shoving it onto this little child who has no idea how to do that." This, they say, of the child who apparently definitively knows that they were meant to be the opposite sex.
One therapist spoke about the difficulty in schools because while schools are "trying to be supportive," and "trying to do the right thing," the schools only have "a little bit of knowledge," and she worries about the "level of binary structure and thinking that happens in the school system."
She said that for parents who go into school for the first kindergarten orientation and find that their child's name has been changed "and they didn't know about it."
"You get the parents who agree and the parents who don't agree, right? I mean, there's that whole issue." For her, and the nodding, agreeing panelists, "we're always working against that heteronormative binary transphobic kind of framework... It's up to us to help parents push against some of that to give their kid as much space as their kid needs to be whatever their kid is going to end up being. And I think if we don't do that, society is going to do it for us."
In conclusion, the panelists discussed how great it was to work with children. "We care about the evidence base, and we care about best practices. And I don't think that we talked nearly enough, though, about joy, and the joy that comes from this work and the joy that our kids, you know, bring to the conversations and lighting up the conversations with families and, and challenging us and pushing us," said the moderator.
This is the discussion Children's Minnesota does not want readers to see.
As a result, The Post Millennial received a legal demand from Children's Minnesota, which publically available information states is the seventh largest pediatric health system in the United States, and advertises as “The Kid Experts.”
WPATH is an international non-profit organization which describes itself as being devoted to transgender health, and The Post Millennial intended to inform readers as to what is going on in the world of trans-affirming mental health care for prepubescent children. It turns out that, according to the panelists, it's an exciting, and burgeoning field. Clinicians from California, Minnesota, and Washington sat on the panel to discuss how they therapeutically treat prepubescent children, including those who are only just verbal, on gender transition.
In response to our news story, which contained a video of the panel as well as a record of the panelists names and their clinics, which they noted at the beginning of the panel, Children's Minnesota, the clinic where the moderator works, reached out to The Post Millennial via an in-house attorney.
Children's Minnesota demanded that the article be deleted from The Post Millennial's website. They did not want the video of the panel where clinicians discussed the medical and therapeutic gender transition of young children to receive broader public attention. We have not deleted the article. The Post Millennial believes that the footage meets every criteria of fair use.
The letter they sent to The Post Millennial stating that the article about the panel "disclosed identifying information of WPATH panelists... without proper consents." The information they objected to was provided in person at the conference, as well as via a live stream of the panel. Children's Minnesota claims that this was a violation of the WPATH Code of Conduct policy. This policy states that "Where applicable, photography, recording, or reproduction of any kind is not permitted without the explicit consent of any person and/or of the author/presenter/copyright- holder(s) of the material being photographed, recorded or reproduced." As such, they claim that our reporting is in violation of the Code of Conduct. After this letter, The Post Millennial took down the video of the full panel and replaced it with a three-minute clip.
The letter was sent by Michael Waldrop, Associate General Counsel for Children's Minnesota, which claims as its mission to "champion the health needs of children and families. We are committed to improving children’s health by providing the highest-quality, family-centered care, advanced through research and education."
Children's Minnesota has a gender clinic, as do many other hospitals across the US, such as Golisano Children's Hospital in Rochester, NY, Columbia University Medical Center, Boston Children's Hospital, Vanderbilt in Nashville, Seattle Childrens, and many more. Children's Minnesota offers confidential gender conversations for children over 10, puberty blockers for children who have already begun the Tanner stage 2 phase of development, and access to cross-sex hormones at about 15 or 16. To begin the process of taking hormones, "a letter of support is required." Fertility preservation is offered as well, since puberty blockers and cross-sex hormones lead to sterility.
The in-house lawyer making the demand against The Post Millennial on behalf of Children's Minnesota, has been active in social media, including taking to Twitter in 2021 to chastise AT&T Stadium in Dallas for allowing the Christian men's group the Promise Keepers to host an event at the stadium. He asked for "Texas queens" to help "stop this event from happening."
Waldrop sent the letter on behalf of Children's Minnesota, presumably because the moderator of the WPATH panel worked at the institution. He was one of four panelists discussing the medical and therapeutic gender transition of children, and gave each panelist an opportunity to introduce themselves at the beginning of the panel, which they did. Waldrop did not immediatley respond to a request for comment from The Post Millennial.
The speakers on WPATH's panel on "Navigating The Changing Landscape With Littles And Their Families: Exploring The Role Of Mental Health Across Different Practice Settings With Transgender And Gender Diverse Pre-Adolescent Children" are clinicians who are excited to work in the burgeoning field of child gender transition. They note that what they call "gender care" began with adults, then branched out to teenagers, and is only now just beginning with children. For these providers, this is a new and exciting space in which to be working.
The panelists are mental health providers, working with children they call "gender expansive," they engage in play with those children during sessions to better understand that gender expression. Yet they don't feel that little kids need therapy for what may be termed "early onset gender dysphoria." Instead, one clinician said that mental health support is provided only as needed, and that usually it is needed not due to gender dysphoria, but because of the social stigma of trans. In other words, it's not the family seeking mental health treatment for a child who plays with supposed opposite-sex toys that's the problem, it's the rest of us.
"The pathology isn't being trans," says one provider, "the pathology is the transphobia that the kids and their families are winding through the world with. And so we're there as a mental health support if that causes really normal stress."
The focus for this clinician is on "helping families—and kids—feel like they can navigate the world with as much confidence, happiness, joy and groundedness as possible."
This, too, is the take of the Columbia University gender clinic, which takes the approach that the mental health issues surrounding the feeling of being born in the wrong body are the fault of society not being accepting enough of people who believe they are born in the wrong body, and not a mental issue with the person experiencing the dysphoria.
A provider who identifies as non-binary, transmasculine and bisexual, agreed with this assessment, saying that much of the work done at their clinic is "parent support and education stuff, too."
This is true "especially when you have two parents that cannot agree on what should happen, that can be like a really tricky situation."
These kinds of "tricky situations" are happening across the country, as one parent dons unicorn glitter pins and rainbow t-shirts, while the other makes the claim that a little girl playing with a toy truck doesn't make her a boy. It is often the more progressive parent that doesn't take the child's interests at face value, and determines that those interests are an indicator of actually, interally being the opposite sex.
Activists have successfully made the switch over the past few years between biological sex and gender identity, and have claimed that gender identity is innate, while biological sex is a social construct. Of course, feminism, where much of this begins, would posit that exactly the opposite is true.
The clinicians reference Dr. Rachel Levine, keynote speaker at the conference, who said that much of the work of trans advocacy and trans medical care was "suicide prevention." The idea has been put forth, with authority, that if children and teens are not permitted to undergo social and medical transition, they will simply kill themselves.
One clinician said that the reason she wanted to work with children was to cure the problems she saw in trans adults. "I worked with so many adults who described their childhood in ways that were very pathologizing, and stigmatizing," she said.
"And out of that they developed a lot of the things that we see happening," she said, "and I really wanted that to be prevented, and not even just prevented, but actually, like, celebrated and, you know, try to really have children, and adolescents be proud of who they are."
The nonbinary, transmasculine clinician uses themselves as an example to kids, and uses their "lived experience" in providing therapy to kids and families.
"I feel lucky to be like in kind of a unique position as a trans clinician to like, be there for the trans kids not just to show like you can grow up and like, have a life and stuff. But then their parents to also get to see like, 'oh, this person is like, professional, sort of.' And then they maybe be less likely to just like dismiss what I have to say, because of the lived experience. Which could also go the other way, sometimes I think."
When doing intake with a "trans kid," this clinician will "want to know about what their goals are that they've identified so far for transition, who's supportive of it? How is it going at school? What our extended family doing?"
Another clinician in Minnesota said that parents are the ones who are signing up their kids for these services. "Kids don't sign up for therapy themselves usually," she said, "so I have usually, really invested parents and kids that have persistently, consistently across many settings been presenting as gender diverse, gender, non binary or trans." She digs into the familiy relationships, and "does alot of drawings, and "sitting on the floor and playing and of course, even with littles I do have time with just the kid so that they can express themselves separate from their families."
She lets parents express their concerns as to their "own transition," and express their "grief" as well. The assumption is that once a child lands in gender care, they are trans, they must be affirmed, parents must adapt to this new reality, even if it has only been perceived by parents watching their kids play with opposite sex toys, or not wanting to wear clothes typically worn by children of their sex, or perhaps just because they like rainbows.
A clinician will often have child patients referred to them by a pediatrician, saying that "a pediatrician is screening for gender diversity within their clinic. And then if the child is expressing some gender diversity, they would refer them to our clinic."
She notes that "something the parents will, the parents always have given approval for that, but they don't always know what the means or who we are or what we're going to do together." Social workers are then sent in to call families and "explain the clinic."
They ask parents their goals for care prior to seeing them at all. And these clinicians make determinations about the family prior to that first appointment. Prior to intake, they "get a sense for where the child and family are at with a kind of understanding their child's gender and what goals they might have for that initial appointment with us."
"That kind of helps prepare us to know what type of room we might be walking into when we see a family for the first time. And then we can differentiate that intake depending on where the child and family are at," she said, noting that this determines whether they treat the child's family as hostile or supportive of gender transition.
"So it might be that we have a really supportive family. And in that case, we're spending time with the child and the family together talking about goals, or we might be that the child and the family are in really different places," she said, in which case they separate the child from the family and encourage the child to be proud to be trans, while reeducating the parents on why gender transition is suicide prevention, or why they need to express and get over their grief, or tell them ways to support their trans child.
"We need to spend a lot of time with the parents for that initial appointment, learning about their fears and concerns and providing a lot of psychoeducation to them at that time," she said.
One clinician does not that "non medical options for some children can be just as affirming as a medical one," and states that not all kids need to go on drugs to be who they truly are.
Another talks about playing games on the floor with kids and discussing fertility issues with them, or telling them not to be afraid of shots.
A clinician from Minnesota spoke about how the role clinicians play with parents, and "being able to correct misinformation." This nonbinary transmasculine therapist related an anecdote in which they told a parent about puberty blockers for their child, and said that therapists should not feel "reluctant to talk about medical stuff" despite not being doctors.
"The other day," they said, "I was talking to a mom and I was like, 'you could try, you know, blockers, you kind of hit the pause button while your kid thinks about it.' And she was like 'you can do what? Oh my God, perfect!'"
The clinician related that they thought "this is a bummer that this had not been like give to you before."
They also spoke about their role in schools, with children's extended family, and their community, and how caregivers can advocate for their "trans kids" across all these areas.
The therapist on the panel determined that she wishes it were possible to "diagnoses the whole family system," especially, she said, when working with kids who are only "recently verbal or just young."
"I do give space for families to work on their own grief and loss around what they thought when they named their kid the name that will not be their name anymore," she said. "And I work with families a lot on their fears for the child because again, what's pathologizing is the transphobia that they're navigating in the world with.
"And so they have some real huge fears. Like they read some article about suicidality and they're like 'my kid's now going to commit suicide.' And so a lot of it is about How to make sure that they're getting support accurate information and really connecting with other families," she said.
She recommends "doctor shopping" for parents when kids are pre-pubertal so that they can begin the medical gender transition process.
She also helps parents figure out how to "go to the school and ask for the right bathrooms," how to "tell the teacher to get the pronouns right," and how to get the child on a sports team based on their gender identity and not their biological sex. She tells parents how to advocate for legal name change, birth certificate change, both in ways that the child does not experience any undue stress. As for grandparents who just don't understand, she said that it's important to figure out "which grandparents love them and which grandparents don't."
She addresses some the medical problems of puberty blockers, saying that fractures could be a problem as bone density decreases as a result of halting the body's natural process, but suggests the kids should just play sports anyway.
One of the Minnesota clinicians emphasized "the importance of like teaching parents how to advocate at school, saying that this is "very important. And it feels like if we are not having them do it, then it's just by not doing it, then the kid is like having to do it. And being really clear with them, like if they're not taking on this emotional labor and work then they're just kind of shoving it onto this little child who has no idea how to do that." This, they say, of the child who apparently definitively knows that they were meant to be the opposite sex.
One therapist spoke about the difficulty in schools because while schools are "trying to be supportive," and "trying to do the right thing," the schools only have "a little bit of knowledge," and she worries about the "level of binary structure and thinking that happens in the school system."
She said that for parents who go into school for the first kindergarten orientation and find that their child's name has been changed "and they didn't know about it."
"You get the parents who agree and the parents who don't agree, right? I mean, there's that whole issue." For her, and the nodding, agreeing panelists, "we're always working against that heteronormative binary transphobic kind of framework... It's up to us to help parents push against some of that to give their kid as much space as their kid needs to be whatever their kid is going to end up being. And I think if we don't do that, society is going to do it for us."
In conclusion, the panelists discussed how great it was to work with children. "We care about the evidence base, and we care about best practices. And I don't think that we talked nearly enough, though, about joy, and the joy that comes from this work and the joy that our kids, you know, bring to the conversations and lighting up the conversations with families and, and challenging us and pushing us," said the moderator.
This is the discussion Children's Minnesota does not want readers to see.
Join and support independent free thinkers!
We’re independent and can’t be cancelled. The establishment media is increasingly dedicated to divisive cancel culture, corporate wokeism, and political correctness, all while covering up corruption from the corridors of power. The need for fact-based journalism and thoughtful analysis has never been greater. When you support The Post Millennial, you support freedom of the press at a time when it's under direct attack. Join the ranks of independent, free thinkers by supporting us today for as little as $1.
Remind me next month
To find out what personal data we collect and how we use it, please visit our Privacy Policy